Overview
Spondylolisthesis is a condition where one of the bones in your spine (a vertebra) slips forward over the one below it. This can sometimes put pressure on nearby nerves, leading to back pain, leg pain, or stiffness.
It most commonly affects the lower back (lumbar spine). While it may sound concerning, many people with spondylolisthesis live active lives. In fact, many cases are mild and can be managed with simple, non-surgical treatments.
Causes
There are different reasons why spondylolisthesis may develop:
- Age-related changes (degenerative type): Natural wear and tear of the joints and discs, usually after age 50.
- Stress fracture (isthmic type): Tiny cracks in a part of the vertebra called the pars interarticularis, often seen in athletes who do repeated back-bending (e.g., gymnastics, cricket fast bowling).
- Congenital (birth defect): Some people are born with a small defect in the spine that allows slipping later in life.
- Trauma: Injury or accident that damages the spine.
- Other causes: Rarely, conditions like tumors or prior spine surgery.
Degenerative spondylolisthesis affects about 5–7% of adults over 50
Signs and Symptoms
Not everyone with spondylolisthesis has symptoms. When present, patients may notice:
- Low back pain – Worsening with activity, relieved by rest.
- Leg pain or sciatica – Pain that radiates down the thighs or legs.
- Numbness or tingling – In the legs or feet due to nerve pressure.
- Tight hamstrings – Difficulty bending forward or standing upright.
- Stiffness or weakness – In more advanced cases.
Rarely, very severe slipping can cause difficulty with bladder or bowel control, which needs urgent attention.
Treatment Options
Conservative (Non-surgical) Management – First Line
Most people with mild to moderate spondylolisthesis improve without surgery. Treatment may include:
- Medications – Pain relievers (acetaminophen, NSAIDs).
- Physiotherapy – Core strengthening, stretching, and posture training.
- Activity modification – Avoiding activities that worsen pain (e.g., heavy lifting).
- Bracing – Sometimes used, especially in young athletes with stress fractures.
- Epidural steroid injections – For persistent leg pain due to nerve irritation.
👉 Research shows that 70–80% of patients with low-grade spondylolisthesis improve with non-surgical treatment
Surgical Options – When Needed
Surgery is considered if:
- Pain does not improve after several months of conservative care.
- There is progressive leg weakness, numbness, or difficulty walking.
- There is significant instability of the spine.
Surgical options include:
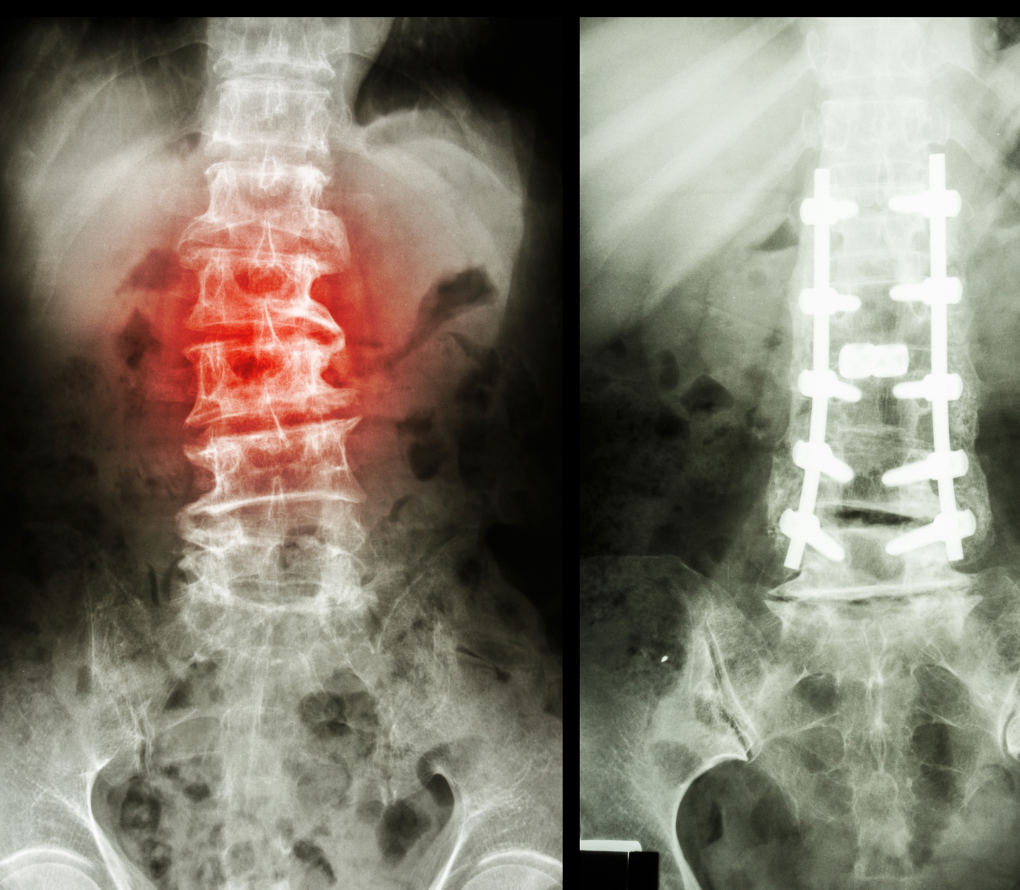
- Decompression surgery (laminectomy/laminotomy): Relieves pressure on the nerves.
- Spinal fusion: Stabilizes the slipped vertebra by fusing it to the bone below.
Surgical outcomes are favorable, with 75–90% of patients reporting long-term relief of pain and improved function.
Frequently Asked Questions
No. Most people do well with non-surgical treatment such as exercise, posture correction, and pain relief. Surgery is only needed in severe or persistent cases.
Many patients feel better within 6–12 weeks, though strengthening the back may take several months.
Yes, but it depends on severity. Many athletes return to sports after rest, physiotherapy, and proper guidance. Your doctor may advise avoiding high-impact sports until pain settles.
In most cases, it is not dangerous and can be well controlled. Rarely, severe nerve compression can cause significant leg weakness or bladder/bowel symptoms, which need urgent care.
Surgery is generally very successful, with around 80–90% of patients reporting significant pain relief and improved quality of life.